Part 6 in our LTC Seating & Positioning series intended to shed some light on the mystery of seating and positioning in the LTC setting. See Part 1, Part 2, Part 3, Part 4, and Part 5. Looking for more information on seating and positioning? Check out our digital, rehab-focused Wheelchair Seating & Positioning Guide here.
What is the pelvis doing?
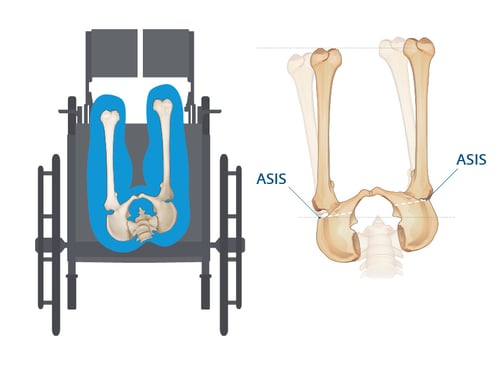
Pelvic rotation is too often confused for a pelvic obliquity. If you were to google “pelvic rotation” or "rotated pelvis" right now, the majority of the images are actually images of a pelvic obliquity. This makes sense, to a degree, because it is very difficult to portray the forward rotation in a drawing. The best angle from which to illustrate a rotated pelvis is from the top, looking down at the pelvis. At this angle, you can clearly see when the ASIS of one side of the pelvis is more forwardly rotated. The image below is displaying a right, (R), rotation as the R side is more forward than the left, (L), side.
A tip that I have for identifying a resident in a pelvic rotation is to consider how much contact is being made with the back support. When a resident presents with a rotated pelvis, one side of the hip will make contact with the back support. On the other side, there will be a gap where the pelvis is more forward. (This is unlike a posterior pelvic tilt where there a gap exists between both sides of the hips and the back support.)
What is going on at the spine?
The spine will follow the rotation of the pelvis. So, if the pelvis presents with a R rotation, then the spine will also rotate to the R.

The head and neck may or may not be affected. If they are impacted, the resident will go into lateral flexion of the neck as if the person is dropping the ear to his or her shoulder. Some forward flexion and rotation of the neck may accompany the lateral neck flexion of the neck.
Wheelchair positioning goals when presented with a pelvic rotation:
Once again, consider if the rotation is fixed or flexible. We should NOT try to correct any abnormality that is fixed, or we will cause undue pain to the resident.
If the rotated pelvis is flexible, the goal can be to correct it, while remembering to take it slowly and to avoid making drastic, sudden changes. Small, incremental changes are best to build up tolerance to the new pelvic alignment. Strive to stabilize the pelvis in the resident’s most neutral alignment with an aggressively contoured cushion:
- A contoured cushion with medial abductors and tapered lateral adductors will create leg troughs for LE alignment and prevent unwanted movement at the pelvis.
- Tapered lateral adductors in conjunction with a deep pelvic well will help to stabilize the pelvis by loading the trochanters and locking in the pelvis to prevent undesirable movement.
- Consider an anti-thrust shelf to reduce forward migration of the pelvis.
If the rotation is fixed, less contour is best because the resident’s unique shape will not fit into a pre-contoured cushion. If you try to force them into a shape unlike their own, pain and pressure on unwanted areas can be created, increasing the risk of wound development.
Look for:
- An immersion-style cushion with less aggressive contouring to protect the bony prominences.
- A cushion with a deep pelvic well to immerse the entire pelvis without causing extra pressure on the ITs.
- A cushion that can be adjusted to compensate for the leg length discrepancy that accompanies a rotation. Measure the longer leg when deciding seat depth for the wheelchair cushion, and ask the cushion manufacturer to customize the length on the shorter side.
At the trunk and head:
- Add stability by using a deeper back support that can immerse the spine and capture the shape of the spinal abnormality. This will also protect the spine from peak pressures that could cause a wound.
- Support the head, if affected. A head support that gives posterior support in the suboccipital area and has angle adjustability to prevent rotation and lateral flexion of the neck is recommended.
So now that you understand what is going on with a pelvic rotation, my hopes are that you will be able to easily identify it on your quarterly screens and during the evaluation. Recognize it, and then go forward using the goals stated above to either correct or accommodate for it according to the standards for flexible or fixed rotation. I assure you, the resident will thank you for it!


Ana Endsjo, MOTR/L, CLT
Clinical Education Manager LTC Division
Ana Endsjo has worked as an occupational therapist since 2001 in a variety of treatment settings. She has mainly worked with the geriatric population, dedicated to the betterment of the treatment of the elderly in LTC centers. Her focus has been on seating and positioning and contracture management of the nursing home resident. With this experience, her hope is to guide other therapists, rehab directors, nurses, and administrators through educational guides, blogs, webinars, and live courses in her role as Clinical Education Manager for the long term care division.